Evolutionarily speaking, we are as a species hardwired to analyze risk based off of information that's directly in front of us--immediately accessible to our five senses. We're designed not to trust food that smells funny, can instantly calculate how far away we should stay from large cats capable of having us for a snack, and do a host of other things that were very useful for us to eke out a living in Olduvai Gorge.
But we live in the 21st century, and nowadays our ability to perceive and estimate risk is hampered by the fact that many of today's risks are abstract, and require a resonably sophisticated understanding of statistics. Take, for example, a recent discussion found in the Paper Of Record about income distribution in the United States. True--it's not really a round table about "risk" per se, unless you consider radically unequal wealth distribution to be a risk to democracy, as Supreme Court Justice Louis Brandeis did when he said that "we can have democracy in this country, or we can have great wealth concentrated in the hands of a few, but we can't have both." Still, the NY Times roundtable was remarkable in that all of the contributors, whether approaching the issue from a left or right viewpoint, agreed that most Americans had vastly underestimated how much wealth is held by relatively few. In particular, a study by Michael Norton and Dan Ariely found that not only do Americans think that wealth distribution to be significantly more equitable than it actually is, but that they would prefer it to be even more equitable than what they (wrongly) perceive.
If this isn't a classic example of what George W. Bush would call "misunderestimation" then it's not clear what is, and moreover, it highlights the difficulties people have in making accurate estimates about things like the distribution of wealth in a hugely complex society: the information simply cannot be found by opening your eyes and looking around. In medicine, we see this all the time: people are often terrified of exotic diseases that pose little threat to them, while being utterly blithe to the daily assaults on their bodies--frequently self-inflicted--that are much more likely to send them six feet under. To wit: drinking, smoking, eating poorly and not exercising.
The recent events at the Fukushima Daiichi nuclear power plant have been a case study in this process of risk assessment, and not altogether surprisingly, we haven't done well collectively in harmonizing our level of panic to the actual threat that the reactors pose. Despite a good number of depressing news stories, some cataloging evasive action by non-Japanese governments, it is far from clear how huge an impact the nuclear accident is going to have. While it is already comparable to the Three Mile Island accident in 1979, and is not (yet) as catastrophic as the Chernobyl accident of 1986, the question still remains: just how dangerous is it? Though the story is far from over there with events taking dramatic swings in short periods, the short answer is something like dangerous, but not as dangerous as you think. Not nearly as dangerous as you think.
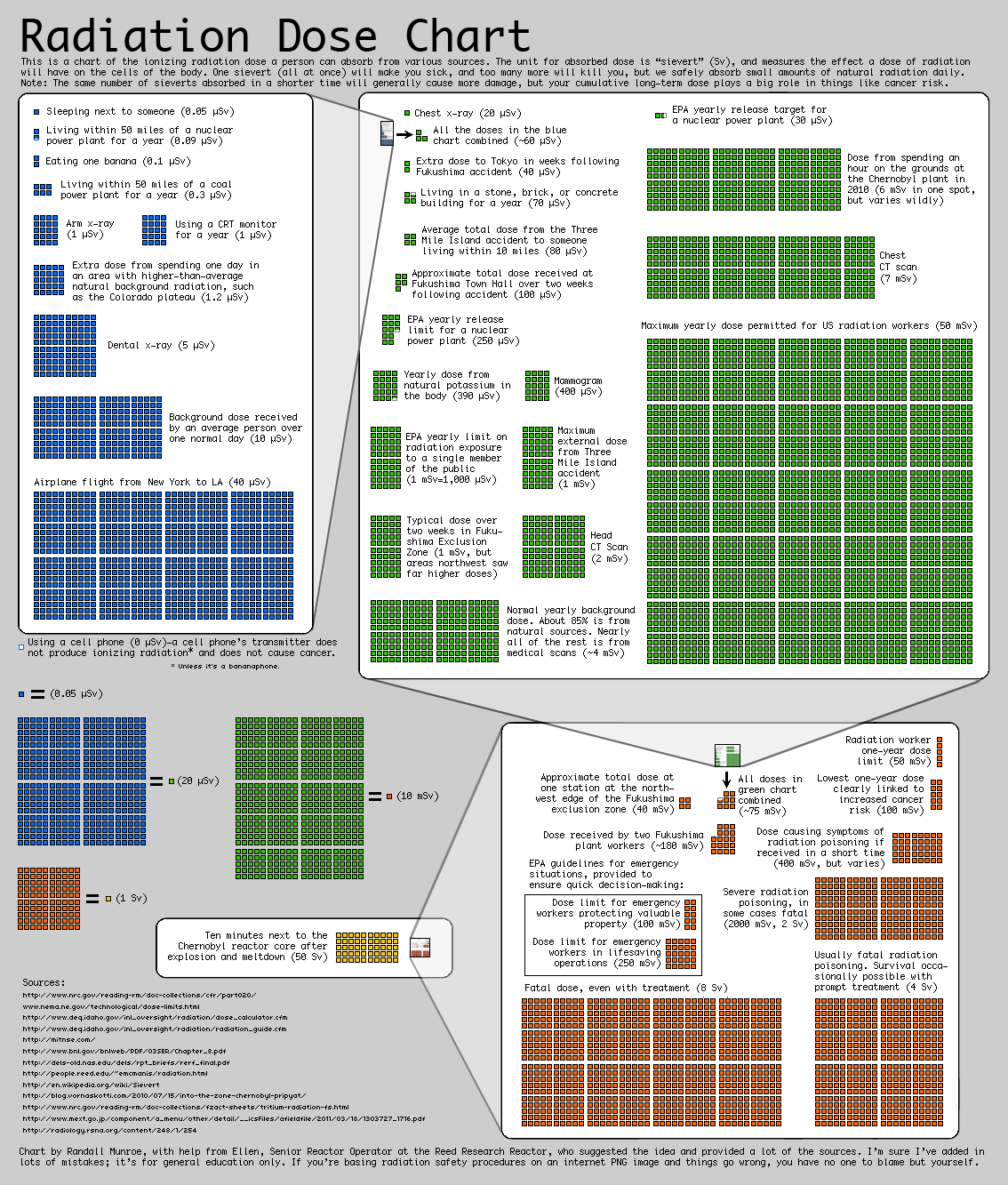
That point is neatly illustrated, both in sound and visual format, in this news story from Adam Ragusea of WBUR (Boston), and is described as the "Dread-to-Risk ratio" by Andrew Revkin of the Dot Earth blog at NYT. Both pieces have the same useful graphic to give you some sense of the relative levels of radiation that we're talking about. Live within 50 miles of a nuclear power plant for one full year? That will give you about 0.1 microSieverts (uSv) of radiation. (What a Sievert is, is a longer discussion, but we'll just shorthand it here and say that it's some relative value of radiation, and that the higher the number, the more dangerous it gets.) One flight from New York to LA buys you about 400 times that amount (40 uSv). That's not even the round trip! A standard chest x-ray, meanwhile, is worth about 20 uSv. But a mammogram is a whopper, clocking in at 3 milliSieverts--thus about 150 "standard" x-rays and just under forty roundtrip flights from NY to LA. A CT scan can be worth almost twice the amount of the mammogram (5.8 mSv).
(In case I've lost some people on this micro/milli distinction, you need 1000 "micros" to make 1 "milli." I'm going to flip back and forth but will point it out when I do.)
So how do these numbers stack up to the nuclear disasters? If you lived within 10 miles of the Three Mile Island plant during the accident and didn't make a run for it, the total dose of radiation you received was 80 microSieverts--far less than one mammogram. By contrast, one area near the Fukushima plant recorded a total dose in one day of 3.6 milliSieverts: less than a CT but more than a mammogram, though of course we're only talking about one day's worth of radiation. With Chernobyl, the radiation levels fluctuated wildly both in time and place so making a general statement about the radiation is essentially impossible, but had you been moved by some weird spirit to take a stroll on the grounds just last year, about 25 years after the accident, you would have gotten two mammograms' worth of radiation for your troubles: 6 milliSieverts. I won't reproduce the pic here out of respect for copyright but highly recommend it to anyone with the time; Ragusea of WBUR translates this into a tone equivalent, and the radiation from TMI is a blip, while the sound for "mammogram" is substantially longer.
I draw two conclusions from all of this. First, while the troubles at Fukushima are by no means trivial, and for that matter aren't yet finished, I think it's a bit premature to write the obituary for nuclear power. In terms of accidents, it's not nearly as dangerous as most people suppose. The problem with nukes, in the TMI and Chernobyl age as well as today, is what to do with the radioactive waste generated by the plants rather than the risks they pose viz. accidents. Second is that we should try to minimize mammograms! Do only the amount that will help save lives, and not one more after that. This was the logic behind the recently revised US Preventative Services Task Force, which recommended no mammograms to women under 50, and biannual ones to those over. Despite this entirely sensible approach--based on good research with a careful eye toward the risk/benefit ratio of the radiation, it should be noted--there were howls of indignation from people purportedly speaking for women, accusing the very bureaucrats who issued the new recs to be female-hostile, or something like that.
--br
(NB--the first draft of this version, which snuck out prematurely, posted some incorrect calculations with respect to x-rays, mammograms, and NY-LA flights. The corrected version is now present.)
Wednesday, March 23, 2011
{kind=link}
Monday, March 21, 2011
The "Back-Door CD4" and Its Ethics, or Lack Thereof
Every year, virtually every first-year medical student gets introduced to medical ethics by learning about the quirky religious beliefs of a small Christian sect: Jehovah’s Witnesses. Based on their interpretation of a passage from Leviticus, Jehovah’s Witnesses consider blood transfusion to be against God’s word, and will thus not accept them, even if their life depends on it. Medical students are introduced to this situation as the classic example of how an American physician is supposed to behave: it don’t matter what your personal beliefs are with respect to the Witnesses, only that you accept their right to their beliefs and, if need be, protect them, defend them, and do whatever else is necessary to let them decide what to do with their bodies. We call that concept informed consent, and it’s the basis of most serious discussions about life-saving medical care in this country. (Of course, I'm talking about adults here; with kids, the situation gets stickier, and with adolescents, stickier still.)
In theory, informed consent is the process by which patients take the reins and make all the genuinely important medical decisions for themselves, while docs serve as something like advisors. Needless to say I’m not talking about the minutiae of medical decision making, like whether to switch a patient from amlodipine to atenolol, but rather the stuff that most patients worry about when they (or their loved ones) walk through the hospital doors: do I want to be resuscitated? do I want to have “everything” done for me? can I refuse some procedures the doctor recommends? These are precisely the kinds of questions where we, as physicians, have an obligation to help patients and their families figure out what they want—that is, not impose on them what we want—and guide them as best we can, even if, indeed, especially if they make decisions that we find shortsighted or wrongheaded or both.
That’s the theory. Fortunately, in terms of practice, most of the time I think we physicians do a pretty admirable job of supporting our patients. You would be hard pressed to find a doctor who thinks it’s acceptable to override the beliefs of a Jehovah’s Witness and force-feed them blood to save their lives. That said, while the core of that philosophy is wholly adopted by the profession, precisely where the boundaries lay can be contentious. And last week I was again reminded that we don’t all agree on what constitutes honoring our patients’ wishes.
It happened when I was hearing about a case of a patient in the Intensive Care Unit fit for an episode of House, M.D. The patient was older without being elderly, and had a respiratory illness that had defied diagnosis despite the best intentions of cardiologists, pulmonologists, infectious disease specialists, and a few other medical professionals to boot. The ID docs, though unsure of what was going on, thought that this was most likely some infection seen in the setting of underlying AIDS, and I, being an ID guy, shared their point of view while hearing the details. Like my colleagues, the question to which I wanted to know the answer was: what was the result of the HIV test? But the patient had adamantly refused HIV testing. And that’s within his right: a doctor can order most blood tests without having to discuss them with a patient, but an HIV test—just like a blood transfusion—is special, and requires a signed form saying that the patient agrees to it. In this case, where a diagnosis of HIV infection might be helpful (more on this later), such a refusal can be maddening. But that is how the rules are set up right now, and once the patient says no, then that’s all she wrote.
However, in this case, that wasn’t all she wrote. HIV is a virus that infects, and destroys, a special kind of white blood cell called a CD4 cell. In general, the further your CD4 cell count drops, the more you are at risk of being infected by the weird organisms that are the sine qua non of AIDS, things like toxoplasmosis, cryptococcosis, penicillium marneffei and a host of other parasites, bacteria and fungi that people with healthy immune systems never develop. A person with a healthy immune system typically has a CD4 count that runs from 500 to 1500, give or take; the definition of AIDS is someone with HIV infection and a CD4 count less than 200.
One of the loopholes of informed consent for HIV testing is that it does not cover CD4 counts.
You can see where this is going. Some doc tried to do an end run around the refusal and checked the patient’s CD4 count. Surprise! It was low, less than 200, although the pattern of the CD4 cells didn’t really look like AIDS (skipping some technical detail here). So then what do you do? You have gotten no closer to the diagnosis, and you have put yourself into the uncomfortable situation where you may be tempted to take action. Sometimes the treatment for some of those weird “opportunistic infections” in AIDS is to just give a person medications for HIV, but you wouldn’t give those meds to a patient without a diagnosis of HIV. In this situation, that wasn’t the case, but what if it were? Would you throw antiretrovirals at the person because his CD4 count was suggestive of HIV—even though the patient unambiguously refused the test? To me, this smells exactly like giving blood to a Jehovah’s Witness: doing what I call a “Back-Door CD4” might seem clever, but it pretty obviously violates the spirit of the patient’s wishes, if not the letter.
Some would argue that the very need to consent people for HIV is outdated. HIV consent was established at a time when the diagnosis was severely stigmatizing, and “positives” could lose jobs, insurance premiums and in general face ostracism from their communities; it also happened at a time when treatment wasn’t exactly effective. Today, the latter is definitely not true, and as I tell my HIV patients all the time, there is no reason to suppose that, should they take their meds every day faithfully, they should live as long as anyone else. Whether the former is true I am a touch skeptical, but I acknowledge that the level of stigma nowhere near approaches where it was twenty years ago. Thus, proponents of the Back-Door CD4 would say that the time for HIV consent has come and gone. Way back in 2004 a doc named LA Jansen wrote in the Journal of Medical Ethics and supposed that the Back-Door CD4 was a form of “conscientious subversion,” something akin to conscientious objection, where a physician acknowledged the existing legal landscape but did his or her own thing based on their personal ethics.
Jansen dresses the term up in calling it “conscientious subversion”; I prefer using simpler language and think of it as a bad idea. By my compass, patients have rights to refuse tests, medications, procedures, and any attempt at thwarting those desires defeats not only the entire point of informed consent, it belies the idea that we are advocates for our patients. Don’t get cute, is what I’d say: we are better than most professions at standing by those we serve. Let’s not mess things up by thinking we know better than they do.
—br
PS—the Jehovah’s Witness example has, for me, not been entirely academic. Twice I have cared for Witnesses who were in situations where transfusion was definitely worth considering, and in one of the cases it was pretty clearly indicated. Like most of my profession, it never entered my mind to try to push the idea on them once I learned of their religious beliefs. For more on Jehovah’s Witnesses and their philosophy behind their refusal of blood transfusions, see here, here and/or here.
In theory, informed consent is the process by which patients take the reins and make all the genuinely important medical decisions for themselves, while docs serve as something like advisors. Needless to say I’m not talking about the minutiae of medical decision making, like whether to switch a patient from amlodipine to atenolol, but rather the stuff that most patients worry about when they (or their loved ones) walk through the hospital doors: do I want to be resuscitated? do I want to have “everything” done for me? can I refuse some procedures the doctor recommends? These are precisely the kinds of questions where we, as physicians, have an obligation to help patients and their families figure out what they want—that is, not impose on them what we want—and guide them as best we can, even if, indeed, especially if they make decisions that we find shortsighted or wrongheaded or both.
That’s the theory. Fortunately, in terms of practice, most of the time I think we physicians do a pretty admirable job of supporting our patients. You would be hard pressed to find a doctor who thinks it’s acceptable to override the beliefs of a Jehovah’s Witness and force-feed them blood to save their lives. That said, while the core of that philosophy is wholly adopted by the profession, precisely where the boundaries lay can be contentious. And last week I was again reminded that we don’t all agree on what constitutes honoring our patients’ wishes.
It happened when I was hearing about a case of a patient in the Intensive Care Unit fit for an episode of House, M.D. The patient was older without being elderly, and had a respiratory illness that had defied diagnosis despite the best intentions of cardiologists, pulmonologists, infectious disease specialists, and a few other medical professionals to boot. The ID docs, though unsure of what was going on, thought that this was most likely some infection seen in the setting of underlying AIDS, and I, being an ID guy, shared their point of view while hearing the details. Like my colleagues, the question to which I wanted to know the answer was: what was the result of the HIV test? But the patient had adamantly refused HIV testing. And that’s within his right: a doctor can order most blood tests without having to discuss them with a patient, but an HIV test—just like a blood transfusion—is special, and requires a signed form saying that the patient agrees to it. In this case, where a diagnosis of HIV infection might be helpful (more on this later), such a refusal can be maddening. But that is how the rules are set up right now, and once the patient says no, then that’s all she wrote.
However, in this case, that wasn’t all she wrote. HIV is a virus that infects, and destroys, a special kind of white blood cell called a CD4 cell. In general, the further your CD4 cell count drops, the more you are at risk of being infected by the weird organisms that are the sine qua non of AIDS, things like toxoplasmosis, cryptococcosis, penicillium marneffei and a host of other parasites, bacteria and fungi that people with healthy immune systems never develop. A person with a healthy immune system typically has a CD4 count that runs from 500 to 1500, give or take; the definition of AIDS is someone with HIV infection and a CD4 count less than 200.
One of the loopholes of informed consent for HIV testing is that it does not cover CD4 counts.
You can see where this is going. Some doc tried to do an end run around the refusal and checked the patient’s CD4 count. Surprise! It was low, less than 200, although the pattern of the CD4 cells didn’t really look like AIDS (skipping some technical detail here). So then what do you do? You have gotten no closer to the diagnosis, and you have put yourself into the uncomfortable situation where you may be tempted to take action. Sometimes the treatment for some of those weird “opportunistic infections” in AIDS is to just give a person medications for HIV, but you wouldn’t give those meds to a patient without a diagnosis of HIV. In this situation, that wasn’t the case, but what if it were? Would you throw antiretrovirals at the person because his CD4 count was suggestive of HIV—even though the patient unambiguously refused the test? To me, this smells exactly like giving blood to a Jehovah’s Witness: doing what I call a “Back-Door CD4” might seem clever, but it pretty obviously violates the spirit of the patient’s wishes, if not the letter.
Some would argue that the very need to consent people for HIV is outdated. HIV consent was established at a time when the diagnosis was severely stigmatizing, and “positives” could lose jobs, insurance premiums and in general face ostracism from their communities; it also happened at a time when treatment wasn’t exactly effective. Today, the latter is definitely not true, and as I tell my HIV patients all the time, there is no reason to suppose that, should they take their meds every day faithfully, they should live as long as anyone else. Whether the former is true I am a touch skeptical, but I acknowledge that the level of stigma nowhere near approaches where it was twenty years ago. Thus, proponents of the Back-Door CD4 would say that the time for HIV consent has come and gone. Way back in 2004 a doc named LA Jansen wrote in the Journal of Medical Ethics and supposed that the Back-Door CD4 was a form of “conscientious subversion,” something akin to conscientious objection, where a physician acknowledged the existing legal landscape but did his or her own thing based on their personal ethics.
Jansen dresses the term up in calling it “conscientious subversion”; I prefer using simpler language and think of it as a bad idea. By my compass, patients have rights to refuse tests, medications, procedures, and any attempt at thwarting those desires defeats not only the entire point of informed consent, it belies the idea that we are advocates for our patients. Don’t get cute, is what I’d say: we are better than most professions at standing by those we serve. Let’s not mess things up by thinking we know better than they do.
—br
PS—the Jehovah’s Witness example has, for me, not been entirely academic. Twice I have cared for Witnesses who were in situations where transfusion was definitely worth considering, and in one of the cases it was pretty clearly indicated. Like most of my profession, it never entered my mind to try to push the idea on them once I learned of their religious beliefs. For more on Jehovah’s Witnesses and their philosophy behind their refusal of blood transfusions, see here, here and/or here.
{kind=link}
Thursday, March 10, 2011
Profile in Courage, Writ Small, But Still
Today was Grand Rounds at my academic medical center. The subject was diabetes and how we--"we" being the medical system as opposed to "we" the individual doctors--can improve outcomes in this disease, which is a killer, and which we (pick whichever "we" you like) stink at treating successfully. The view of the speakers, with which I'm sympathetic, is that we require less gee-whiz bioscience breakthroughs than we do a comprehensive, systematic plan for identifying, following, and ensuring affected patients stay on their meds. None of their suggestions were particularly sexy and didn't involve lots of fancy technology except for using a personal computer. I was persuaded by their assertion that sometimes it's simple but labor-intensive solutions in medicine that are the ones with the best chance of success.
Grand Rounds at my hospital always begins with a physician "presenting a case." Typically this involves a resident summarizing a bare-bones medical history of some patient who has some affliction related to the topic being discussed: gout, Wegener's granulomatosis, multiple myeloma, sepsis, a heart attack, you name it. Often the speaker will make some remark about the case in relation to his or her talk, and then it's on with the show. This kind of case presentation is de rigueur among physicians, and after one has lived & breathed medicine for long enough (i.e. survived the third year of medical school), one becomes so acclimated to the rhetorical form that one can get fairly desensitized to the reality that it's actual human beings that are being spoken of.
I don't mean to imply that physicians speak about patients in a de-humanizing way when a case is presented--that's never acceptable--only that the process of summary and discussion of history, physical exam, and laboratory findings in the dry, sterile, & detached form of the "case presentation" is second-nature to physicians, and must be creepy as hell to patients if they had to listen to themselves being discussed. Sometimes I try to teach residents and students at the bedside in the old-fashioned manner, but I always make sure to alert patients that such feelings might overtake them as I "do some doctor-talk with my colleagues." I do everything I can think of to make that moment as comfortable as possible for patients, but ultimately my suspicion is that all my efforts, at best, help blunt the sense of creepiness rather than remove it altogether.
So you can imagine what it must have felt like for the gal today to have her case of diabetes discussed in the amphitheater filled with well over 100 physicians in attendance, watching the medical facts of her life, neatly summarized into three Power Point slides, as she sat in the fifth row. I've been part of this community for more than ten years now and I still get nervous when facing the White Coat Army en banc; I can only imagine how intimidating that must have felt for her. Then, at the end of the presentation, the presenter noted to the crowd that the patient was in attendance, and asked her if she had any thoughts to add. Again, with what I would describe as remarkable poise, she eloquently explained some of the life circumstances that made her choose treatment options that, without that critical context, would puzzle and frustrate physicians.
She not only did this, but managed to deliver an observation with a small barb attached to the end of it: "I see that many of you here are eating really nice lunches here today, really healthy food. Well, my family has to live month-to-month because of our income, and I can tell you that a pound of pasta and some tomato sauce goes a lot further than some other food." It was a complex observation, but the sheer nerve & determination it took to march into what could very well have felt like a Lion's Den, and deliver that speech with such clarity, was quite a thing to watch. (Disclosure: lunches are not sponsored by anyone at our medical center. Mostly this woman was referring to tasty-but-modestly-sized deli sandwiches using fresh ingredients and a fruit salad.)
It's very unusual to invite patients to hear their own cases discussed in this kind of format, weirder still to give them a platform for a few minutes to speak about their challenges. Certainly in this setting it was a brilliant idea to include such a patient in the dialogue: my school gets an "A" not merely for effort but execution as well! Though at the end of the day, when the speaker concluded the lecture and the audience gave its polite applause per the cultural conventions of Grand Rounds, no one thought to give a special thanks for this woman. On that count, I think the organizers earned a D-minus.
Grand Rounds at my hospital always begins with a physician "presenting a case." Typically this involves a resident summarizing a bare-bones medical history of some patient who has some affliction related to the topic being discussed: gout, Wegener's granulomatosis, multiple myeloma, sepsis, a heart attack, you name it. Often the speaker will make some remark about the case in relation to his or her talk, and then it's on with the show. This kind of case presentation is de rigueur among physicians, and after one has lived & breathed medicine for long enough (i.e. survived the third year of medical school), one becomes so acclimated to the rhetorical form that one can get fairly desensitized to the reality that it's actual human beings that are being spoken of.
I don't mean to imply that physicians speak about patients in a de-humanizing way when a case is presented--that's never acceptable--only that the process of summary and discussion of history, physical exam, and laboratory findings in the dry, sterile, & detached form of the "case presentation" is second-nature to physicians, and must be creepy as hell to patients if they had to listen to themselves being discussed. Sometimes I try to teach residents and students at the bedside in the old-fashioned manner, but I always make sure to alert patients that such feelings might overtake them as I "do some doctor-talk with my colleagues." I do everything I can think of to make that moment as comfortable as possible for patients, but ultimately my suspicion is that all my efforts, at best, help blunt the sense of creepiness rather than remove it altogether.
So you can imagine what it must have felt like for the gal today to have her case of diabetes discussed in the amphitheater filled with well over 100 physicians in attendance, watching the medical facts of her life, neatly summarized into three Power Point slides, as she sat in the fifth row. I've been part of this community for more than ten years now and I still get nervous when facing the White Coat Army en banc; I can only imagine how intimidating that must have felt for her. Then, at the end of the presentation, the presenter noted to the crowd that the patient was in attendance, and asked her if she had any thoughts to add. Again, with what I would describe as remarkable poise, she eloquently explained some of the life circumstances that made her choose treatment options that, without that critical context, would puzzle and frustrate physicians.
She not only did this, but managed to deliver an observation with a small barb attached to the end of it: "I see that many of you here are eating really nice lunches here today, really healthy food. Well, my family has to live month-to-month because of our income, and I can tell you that a pound of pasta and some tomato sauce goes a lot further than some other food." It was a complex observation, but the sheer nerve & determination it took to march into what could very well have felt like a Lion's Den, and deliver that speech with such clarity, was quite a thing to watch. (Disclosure: lunches are not sponsored by anyone at our medical center. Mostly this woman was referring to tasty-but-modestly-sized deli sandwiches using fresh ingredients and a fruit salad.)
It's very unusual to invite patients to hear their own cases discussed in this kind of format, weirder still to give them a platform for a few minutes to speak about their challenges. Certainly in this setting it was a brilliant idea to include such a patient in the dialogue: my school gets an "A" not merely for effort but execution as well! Though at the end of the day, when the speaker concluded the lecture and the audience gave its polite applause per the cultural conventions of Grand Rounds, no one thought to give a special thanks for this woman. On that count, I think the organizers earned a D-minus.
Wednesday, March 2, 2011
BRB Link Dump
My spiritual and theological leanings are probably just enough to drive everyone concerned totally nuts: I am intellectually atheist, though functionally Jewish, plus I'm fond of various other religions (or at least certain aspects of them). We have a new Rabbi at our Synagogue and while he appears to be a very charismatic man, my own religious leanings are such that I do not look to him for spiritual leadership in any capacity, and I remain a member partly because I like going to synagogue, but mostly because I really like peace between me and my wife.
The point of this rambling being that although I long ago decided to follow my own path and look toward no other man or woman as my spiritual leader, if I had to choose a person, I quite possibly could have chosen Peter Gomes, whose life ended just a little too soon for my tastes earlier this week. Gomes was about the most polar opposite person you could pick for me to follow: he was African-American; I was white. He was Christian; I, an agnostic Jew. He was gay; I, not so much, thanks, though as Jerry Seinfeld noted, not that there's anything wrong with that. He was, for most of his life, a Republican, and I have mostly not been a Democrat because I regarded them as too far to the right. He was something of a dandy with something of a pompous manner of speaking at the most Establishment university in the United States; I am a well-educated though frequently unspeakably crude dude who went to Abbie Hoffman's school and often sneers at The Establishment. On the surface, thus, not my kind of guy.
But once you peel away his formal and sometimes antiquated mannerisms and really listen to Peter Gomes, there is aught but beauty, truth, and light. Here is a brief comment on gay marriage, while here a longer talk with Charlie Rose. He opens the conversation with Rose with a line that elegantly encapsulates why I find him so admirable: "I like the notion that there is much yet to be revealed about the Christian faith; it's not all over yet. It's not a complete story, and we're moving into it. There is much yet to be revealed, and I think our best theological days are ahead of us." If that ain't a bare-bones summary of the philosophy of the great Talmudic masters (that is, the part of the Talmudic masters that I find worthy of attention), then I don't know what is. I have not read any of his books, and my acquaintance with him is largely through talks & other coverage he's received in that peculiar Harvardo-centric fishbowl of Boston media (you could catch his sermons on Sunday morning on WHRB, the Harvard radio station). It may be a tough pill for me to swallow to read a book about Jesus, but in the coming months I may peruse one of his books to stay connected with this eminently decent and astonishingly eloquent man.
More immediate concerns that nobody else in the vicinity of Harvard Yard prematurely join the Reverend Gomes are very much on the minds of Massachusetts public health officials as they scramble to contain a measles outbreak inflicted on the city by an unvaccinated French woman working for the French consulate downtown. What a mess: the super-contagious virus may have spread to a professor at UMass Boston, and thus his students are bearing the brunt of some public health measures, but fortunately seem not to be too bothered by the whole fuss. Though make no mistake, a fuss this is: measles spreads like wildfire and--while not overwhelmingly lethal by Andromeda-strain standards--kills simply by the fact that so many can become infected so quickly. Even a low mortality rate of, say, three percent can be a lot of bodies if tens of thousands become infected. And while the vaccine for measles (the "MMR") is good, it's not perfect, so even vaccinated people are at risk of infection, especially if they haven't been vaccinated in decades. As I noted in a previous entry: this virus is a killer. How this gal got into the US and was allowed to work without having a documented MMR is not fully clear to me, but many are paying the price for her folly.
--br
The point of this rambling being that although I long ago decided to follow my own path and look toward no other man or woman as my spiritual leader, if I had to choose a person, I quite possibly could have chosen Peter Gomes, whose life ended just a little too soon for my tastes earlier this week. Gomes was about the most polar opposite person you could pick for me to follow: he was African-American; I was white. He was Christian; I, an agnostic Jew. He was gay; I, not so much, thanks, though as Jerry Seinfeld noted, not that there's anything wrong with that. He was, for most of his life, a Republican, and I have mostly not been a Democrat because I regarded them as too far to the right. He was something of a dandy with something of a pompous manner of speaking at the most Establishment university in the United States; I am a well-educated though frequently unspeakably crude dude who went to Abbie Hoffman's school and often sneers at The Establishment. On the surface, thus, not my kind of guy.
But once you peel away his formal and sometimes antiquated mannerisms and really listen to Peter Gomes, there is aught but beauty, truth, and light. Here is a brief comment on gay marriage, while here a longer talk with Charlie Rose. He opens the conversation with Rose with a line that elegantly encapsulates why I find him so admirable: "I like the notion that there is much yet to be revealed about the Christian faith; it's not all over yet. It's not a complete story, and we're moving into it. There is much yet to be revealed, and I think our best theological days are ahead of us." If that ain't a bare-bones summary of the philosophy of the great Talmudic masters (that is, the part of the Talmudic masters that I find worthy of attention), then I don't know what is. I have not read any of his books, and my acquaintance with him is largely through talks & other coverage he's received in that peculiar Harvardo-centric fishbowl of Boston media (you could catch his sermons on Sunday morning on WHRB, the Harvard radio station). It may be a tough pill for me to swallow to read a book about Jesus, but in the coming months I may peruse one of his books to stay connected with this eminently decent and astonishingly eloquent man.
More immediate concerns that nobody else in the vicinity of Harvard Yard prematurely join the Reverend Gomes are very much on the minds of Massachusetts public health officials as they scramble to contain a measles outbreak inflicted on the city by an unvaccinated French woman working for the French consulate downtown. What a mess: the super-contagious virus may have spread to a professor at UMass Boston, and thus his students are bearing the brunt of some public health measures, but fortunately seem not to be too bothered by the whole fuss. Though make no mistake, a fuss this is: measles spreads like wildfire and--while not overwhelmingly lethal by Andromeda-strain standards--kills simply by the fact that so many can become infected so quickly. Even a low mortality rate of, say, three percent can be a lot of bodies if tens of thousands become infected. And while the vaccine for measles (the "MMR") is good, it's not perfect, so even vaccinated people are at risk of infection, especially if they haven't been vaccinated in decades. As I noted in a previous entry: this virus is a killer. How this gal got into the US and was allowed to work without having a documented MMR is not fully clear to me, but many are paying the price for her folly.
--br
Subscribe to:
Posts (Atom)